Retake
N9) Fever, headache, and neck stiffness
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with headache.
- Review the DDx considerations in a patient with headache.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with headache.
History
A 55-yo woman presents to the ER with a progressive, severe headache, fever, photophobia, and neck stiffness over the past three days. Her husband claims she has been making odd comments for the past hour and decided to bring her to the ER. She has a history of HIV and HSV-2.
Physical Exam
BP: 105/70 mmHg , HR 85 BPM , RR 30 BPM, Temp 102F, O2 saturation 95%.
Vital Signs: BP 145/90, HR 105, RR 22, Temp 101.8°F, SpO2 97% on room air.
General: The patient is in moderate distress, appears fatigued and diaphoretic.
HEENT: Pupils equal, round, and reactive to light. Kernig’s and Brudzinski’s sign is present.
Neurological: Alert and oriented x3, cranial nerves II-XII intact, strength 5/5 in all extremities, sensation intact, deep tendon reflexes 2+ and symmetric, negative Babinski.
Labs
CBC: WBC 12,000/mm3,
HSV-2 PCR: Positive,
HIV viral load: 250,000 copies/mL, CD4 count: 100 cells/mm3
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient's symptoms, including headache, fever, neck stiffness, photophobia, coupled with a positive Kernig's and Brudzinski's signs on physical exam, and a history of untreated HIV and HSV-2, make meningitis the most likely diagnosis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
In this patient with poorly controlled HIV, a CT head is needed to rule out complications like space-occupying lesions, more common in immunocompromised patients, before performing a lumbar puncture for meningitis diagnosis. Large intracranial space-occupying lesions can cause brain herniation if a lumbar puncture is performed. However, in a patient without red flags such as focal deficits, altered mental status, increased intracranial pressure, new seizures, immunocompromised status, CNS disease history, or older age, a CT head may not be required initially.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
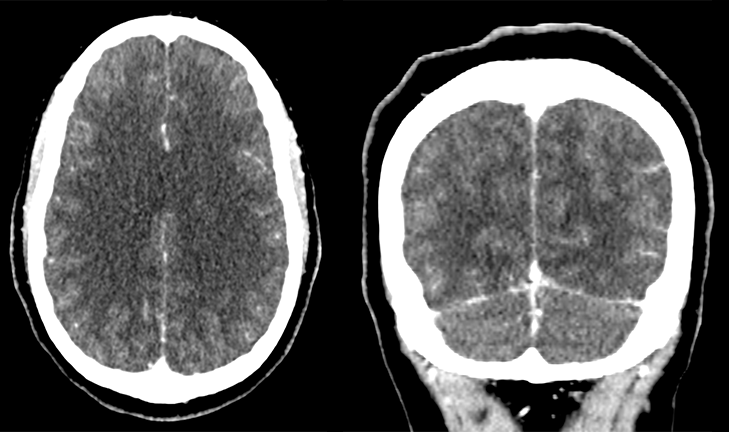
CT head with and without IV contrast
Which of the following describes the findings from the head CT scan?
Minimal leptomeningeal enhancement is present in several parietal-occipital sulci. These findings are consistent with meningitis in this clinical context.
Is there a space-occupying lesion detected in the CT scan?
The CT scan does not show any space-occupying lesion that would contraindicate a lumbar puncture.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is required.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s clinical presentation and imaging findings are consistent with meningitis.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
A 55-year-old immunocompromised woman with uncontrolled HIV presents with symptoms including headache, fever, neck stiffness, and photophobia. To rule out space-occupying lesions that would contraindicate a lumbar puncture, a CT scan was performed, which revealed leptomeningeal enhancement, confirming the meningitis diagnosis. A lumbar puncture should be performed to establish the diagnosis and identify the causative organism. The patient should be admitted to the hospital and started on empiric therapy, along with antipyretics and analgesics. The CSF culture results from the lumbar puncture will guide targeted therapy against the specific organism. Consultation with infectious disease specialists is advised for antiretroviral therapy and HIV management. The patient should also receive counseling on adhering to antiretroviral therapy and work with a social worker to address any barriers to care. Following discharge, arrangements should be made for outpatient follow-up with the primary care provider to ensure ongoing management of HIV and meningitis.
Lessons Learned:
- The gold standard diagnostic method for meningitis remains a lumbar puncture. This procedure allows for the collection of cerebrospinal fluid (CSF) and analysis of its contents, including cell count, protein and glucose levels, as well as the identification of the causative organism through culture and sensitivity testing. The culture results obtained from the lumbar puncture guide appropriate antibiotic management tailored to the specific pathogen.
- Imaging has a limited direct diagnostic value in cases of meningitis. However, CT plays a crucial role in patients with certain risk factors such as an immunocompromised state, history of mass lesion or stroke, new onset seizures, papilledema, altered consciousness, focal neurologic deficit, focal deficits, altered mental status, increased intracranial pressure, new seizures, CNS disease history, or older age. These conditions warrant a CT scan to rule out space-occupying lesions that may contraindicate a lumbar puncture due to the risk of brain herniation.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}